🧠 Neuroendocrinology Clinical Case
♂ Male, 42 yrs Acromegaly
🔬 GH + IGF-1 elevated Microadenoma 7×6 mm
🔪 Transsphenoidal Surgery Hypophysectomy
✅ DM remission HTN reversal
💊 Medications discontinued Post-op
Background & Case Presentation
📋
IntroductionBackground & Clinical Significance
Acromegaly is a rare endocrine disorder caused by chronic excess secretion of growth hormone (GH), almost always from a pituitary adenoma. It carries a significantly elevated burden of cardiovascular, metabolic, and respiratory comorbidities.
Both type 2 diabetes mellitus (T2DM) and hypertension are well-recognised secondary complications of GH/IGF-1 excess, arising through insulin resistance, sodium retention, and direct vascular remodelling.
The critical clinical question: Can early surgical cure of GH excess reverse established cardiometabolic comorbidities — eliminating the need for lifelong pharmacotherapy?
Pathophysiology: Excess GH → ↑ hepatic IGF-1 → insulin resistance, gluconeogenesis, sodium retention → T2DM & hypertension. Surgical normalisation of GH/IGF-1 interrupts this cascade, allowing metabolic recovery.
Rare: 3–4/million/year
Avg delay to Dx: 7–10 yrs
Micro vs Macro adenoma
CVD leading cause of death
👤
Case PresentationClinical History & Examination
42
Age (Male)
T2DM +
HTN
Recent-onset
comorbidities
7×6
mm
Microadenoma
(MRI confirmed)
Presenting Complaints
→Breathlessness on exertion
Clinical Examination — Acromegaly Stigmata
🫂
Coarse Facies
Frontal bossing, prognathism
🤲
Acral Enlargement
Large hands & feet
🏷️
Skin Tags
Multiple, distributed
Investigations
🔬
BiochemistryHormone & Metabolic Workup
Pre-operative Values
Growth Hormone (GH)
↑ Elevated
Ref: <1 μg/L
IGF-1
↑ Elevated
Age-adjusted
Fasting Blood Glucose
↑ Diabetic range
>126 mg/dL
Blood Pressure
↑ Hypertensive
>140/90 mmHg
Post-operative Normalisation
Growth Hormone (GH)
→
✓ Normal
IGF-1
→
✓ Normal
Blood Glucose
→
✓ Normalized
Blood Pressure
→
✓ Normalised
GH nadir during OGTT <1 μg/L defines biochemical cure. Both GH and IGF-1 normalised post-operatively, confirming surgical remission.
🧲
ImagingMRI Pituitary — Findings
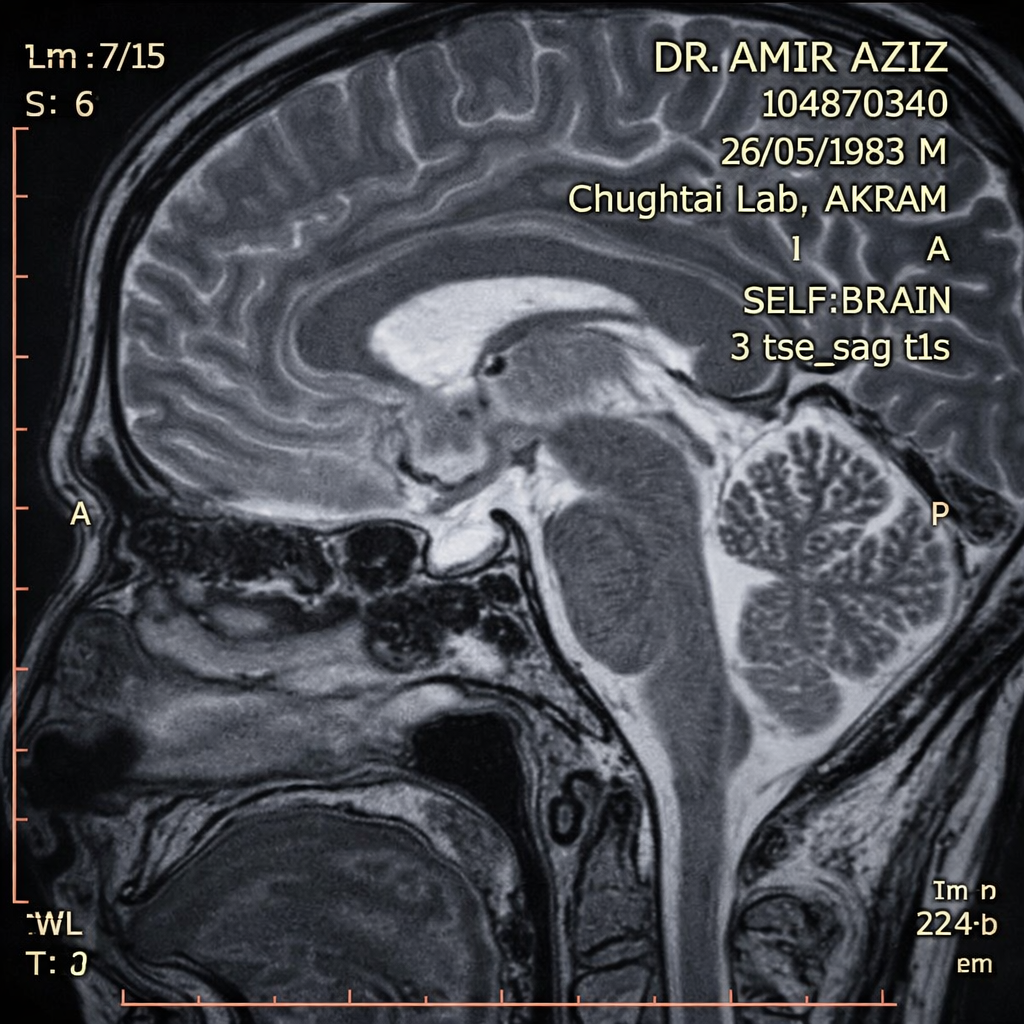
Schematic representation — not to scale
| MRI Finding | Description |
|---|
| Lesion type | Microadenoma (<10mm) |
| Dimensions | 7 × 6 mm |
| Location | Pituitary gland |
| GH-secreting | Confirmed |
| Cavernous sinus | Not invaded |
| Optic chiasm | Not compressed |
Microadenoma (<10mm) carries higher remission rates with transsphenoidal surgery vs. macroadenoma. Absence of cavernous sinus invasion is a favourable prognostic indicator.
⚡
Disease BurdenSystemic Impact of GH Excess
GH Hypersecretion
↑ Hepatic IGF-1 production, insulin antagonism
↓
T2DM
Insulin resistance, gluconeogenesis ↑
Hypertension
Na+ retention, vascular remodelling
↓
Cardiovascular Sequelae
Breathlessness, chest discomfort, fatigue
| Complication | Pre-op | Post-op |
|---|
| T2DM | Present | Resolved ✓ |
| Hypertension | Present | Resolved ✓ |
| Anti-diabetic Rx | Required | Discontinued ✓ |
| Antihypertensive Rx | Required | Discontinued ✓ |
Management & Outcome
🔪
ManagementTranssphenoidal Hypophysectomy
Surgical Approach
①Route: Transsphenoidal (endonasal endoscopic)
②Target: Selective adenomectomy — 7×6mm lesion
③Goal: Biochemical cure (GH nadir <1 μg/L post-OGTT)
✓Outcome: Complete tumour resection achieved
Why Microadenoma Favourable?
•Higher remission rate (70–90%) vs macroadenoma
•No cavernous sinus or optic chiasm involvement
•Clear surgical margins achievable
•Lower risk of pituitary insufficiency post-op
Post-Operative Course
Immediate Post-op
GH and IGF-1 levels began to decline. Patient monitored in post-surgical endocrine unit.
Early Follow-up
Significant improvement in blood glucose and blood pressure. Dose reduction of medications initiated.
Biochemical Cure Confirmed
GH and IGF-1 normalised. Both antidiabetic and antihypertensive medications fully discontinued.
💬
DiscussionKey Learning Points
⚠️ Diagnostic Delay: The Hidden Risk
The mean delay from symptom onset to acromegaly diagnosis is 7–10 years. New-onset T2DM or hypertension with somatic changes — coarse facies, acral enlargement, skin tags — should prompt GH/IGF-1 screening before attributing the metabolic disorder to primary disease.
🔵 Acromegaly as Reversible Cause of T2DM
GH excess causes insulin resistance that fully resolves with biochemical cure. This case confirms that T2DM secondary to acromegaly is a functional metabolic state — not structural — and is surgically reversible in the microadenoma setting.
✅ Microadenoma: Optimal Surgical Outcome
The 7×6mm size and absence of invasive features placed this patient in the high-cure-probability category. Transsphenoidal surgery achieved complete remission, demonstrating the power of early detection in preventing irreversible comorbidity.
🟣 Cardiometabolic Disorders as Sentinel Signs
Breathlessness, fatigue, and chest discomfort alongside new-onset diabetes and hypertension in a middle-aged male with physical stigmata of acromegaly represents a recognisable — but often missed — clinical constellation. Endocrinological workup should be routine in such presentations.
🏥
Clinical PearlWhen to Screen for Acromegaly
| Screening Trigger | Relevance |
|---|
| New-onset T2DM + somatic changes | High yield |
| Resistant hypertension, young age | High yield |
| Multiple skin tags + coarse features | Moderate |
| Enlarged shoe/ring size (history) | Moderate |
| Carpal tunnel syndrome | Supportive |
| Sleep apnoea + metabolic syndrome | Supportive |
Screening test: Serum IGF-1 (age/sex-adjusted). If elevated → GH suppression OGTT for confirmation. MRI pituitary if biochemically confirmed.
Conclusion
Biochemical Cure
GH + IGF-1
Normalised post-transsphenoidal hypophysectomy for a 7×6mm GH-secreting microadenoma, confirming complete surgical remission — the primary goal of acromegaly management.
DM Remission
Full Reversal
Type 2 diabetes mellitus secondary to GH-induced insulin resistance resolved entirely post-operatively. All antidiabetic medications discontinued without recurrence.
HTN Reversal
Medications Off
Hypertension driven by sodium retention and vascular remodelling from GH excess reversed after biochemical cure. Antihypertensive therapy fully discontinued post-op.
Keywords:
Acromegaly
Pituitary Microadenoma
Diabetes Remission
Hypertension Reversal
Growth Hormone Excess
Transsphenoidal Surgery
IGF-1
Biochemical Cure
Neuroendocrinology
COI Declaration
Conflict of Interest: The authors declare no conflict of interest. Informed consent was obtained from the patient for publication of this case report. No commercial funding was received. Institutional ethics approval obtained for case report publication.
Do Not Cover This Area
Reserved by Secretariat — per ICE 2025 Poster Presenter Guidelines (30 cm)
.png)

 Address:
Address:
 Phone:
Phone:
 Email:
Email: